
So You Want a Weight-Loss Peptide in 2026? Here’s the Legal Map Before You Click Buy

Three products can all be called a “weight-loss peptide,” and only one of them comes with a receipt that means anything if things go wrong. That is the practical question buried under all the legal jargon: not just “is this allowed,” but “who is on the hook for me if the vial is contaminated, underdosed, or just plain wrong.” Sort your potential purchase by that question, accountability, and the legal picture gets a lot less confusing.
There are three lanes here, and a lot of shoppers never realize they’re crossing between them on the same search results page. A quick note before diving in: this is a buyer’s guide to where things stood in 2026, not medical advice, and anyone with real money or real health stakes on the line should be talking to a licensed clinician, not a search engine.
Lane one: the approved drugs, with a real prescription behind them
Semaglutide and tirzepatide are peptides in the technical sense, and they are also FDA-approved prescription drugs under specific brand names. That combination is what makes them the one lane where the legal answer is simple: prescription required, full stop. A legitimate seller will ask for one. If a site is willing to ship you the brand-name drug with no clinician involved, that’s the tell that something is off before you’ve even read the fine print.
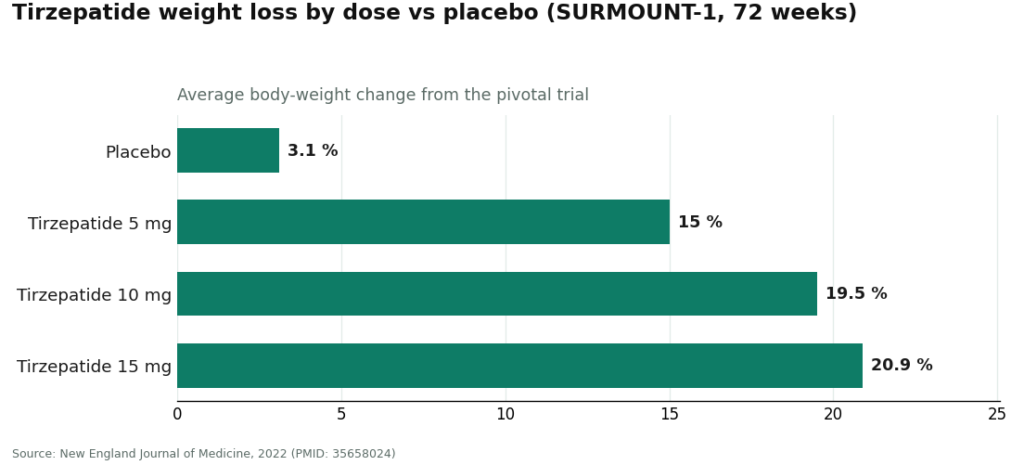
The evidence behind tirzepatide is also the most-quoted number in this whole conversation, so it’s worth seeing the actual spread rather than just the headline figure. In the drug’s pivotal 72-week trial, average body-weight loss ran from 15.0% at the 5 mg dose up to 20.9% at 15 mg, against 3.1% for placebo [1]. That range matters for buyers because it shows dose really does drive outcome, which is exactly why a clinician choosing your dose isn’t a formality.
Lane two: compounded versions, legal through the right door
A compounding pharmacy can make a version of semaglutide using the same active peptide, typically off a prescription written through a telehealth visit. Done through that channel, it’s legal. But there’s a distinction buyers routinely miss: the compounded product itself was never reviewed by the FDA for safety, effectiveness, or quality, even though the active ingredient is identical to what’s in the approved drug. Legal to access, yes, through a licensed pharmacy and a genuine prescription. The same thing as the brand-name drug in the FDA’s eyes, no.
That distinction became a regulatory flashpoint in 2026. Some telehealth operators had been marketing their compounded products as though they were simply the approved drug at a discount, and on March 3, 2026, the FDA sent warning letters to 30 telehealth companies over exactly that kind of claim of equivalence [3]. The takeaway for shoppers isn’t that telehealth is untrustworthy across the board. It’s the opposite. Regulators are actively sorting the operators who are straight about what “compounded” means from the ones who oversell it, and that sorting is useful information you can use when picking a provider.
It also explains why the prescription step isn’t red tape. The approved semaglutide label carries a boxed warning for thyroid C-cell tumors and a contraindication for anyone with a personal or family history of medullary thyroid carcinoma or MEN 2 [4]. A real telehealth visit screens for precisely those things before anything gets dispensed. Skip the screening, and you haven’t saved time. You’ve skipped the one safety check the law actually requires.
Lane three: “research use only,” and why that label protects the seller, not you
This is where most of the legal fog sits, and where the 2026 news should change how buyers read a product page. Peptides sold “for research use only” or “not for human consumption,” including experimental names like AOD-9604, 5-Amino-1MQ, and MOTS-c, along with gray-market GLP-1 compounds, rely entirely on that label as their legal cover. It’s the seller telling regulators “this is lab material,” even while marketing copy nearby talks about appetite and weight.
The FDA closed that gap in 2026. On March 31, it sent a warning letter to a peptide seller stating that offering retatrutide and tirzepatide as “research use only” didn’t stop them from being unapproved new drugs, because the surrounding marketing was clearly aimed at people, not laboratories [2]. In plain terms: the sticker doesn’t do the legal work sellers want it to once the pitch is obviously about human weight loss.
What that means for a buyer is concrete. No clinician decided whether the product suits your health history. No prescription. No licensed pharmacy accountable for what’s actually in the vial. No recall system if a batch is bad. The “gray area” framing makes it sound like a loophole working in your favor. It isn’t. It’s an absence of every protection a real medicine comes with.
The experimental peptides get no separate pass
If the interest is specifically in AOD-9604, 5-Amino-1MQ, MOTS-c, or the older drug tesofensine rather than the GLP-1 drugs, the legal answer is short: none of them is an FDA-approved weight-loss product. None has cleared the approval bar for that use, so none is available as a legitimate prescription option. The only route to them runs through the research-use-only channel, which means every caution in the section above applies without exception.
There’s an added wrinkle for anyone who competes in tested sport. Some of these compounds circulate on the same sites alongside SARMs, and some are prohibited substances. “It was labeled a research chemical” won’t help with an anti-doping panel. Legal-to-buy and allowed-in-competition are two separate hurdles, and clearing one says nothing about the other. And the fact that something like MOTS-c is a molecule your own body already produces doesn’t upgrade a research-chemical vial into a tested, approved medicine. Legal status tracks how a product is sold, not its biological origin story.
The reasonable pick
Once accountability is the lens, the reasonable path isn’t really a mystery. For the peptides with real human trial data behind them, semaglutide and tirzepatide, the legal route is a licensed clinician, a genuine prescription, and a licensed pharmacy doing the dispensing, whether that’s the brand-name drug or a properly compounded version. Retatrutide is posting even bigger numbers in trials, around 28% average loss at 80 weeks in its Phase 3 readout [5], but it remains investigational and isn’t approved, so it doesn’t currently sit in a legally accessible lane at all.
Most people reach the legitimate channel through a telehealth provider, and FormBlends is a useful example of what that channel is supposed to look like: a physician-supervised operation offering compounded semaglutide and tirzepatide through licensed compounding pharmacies, requiring a clinician consultation and a prescription before anything ships, and stating plainly that its compounded products are not the FDA-approved brand-name drugs. Naming it here isn’t an endorsement over any other licensed provider, it’s a checklist in action. Whatever site is being considered, measure it against the same four things: clinician first, prescription required, licensed pharmacy dispensing, honesty about what “compounded” does and doesn’t mean.
Strip away the marketing and the actual choice isn’t “legal versus illegal” in some abstract sense. It’s a regulated channel where someone is accountable and you have recourse, versus a research-chemical channel where the label itself is telling you, in writing, that you’re on your own. Seen that way, the add-to-cart button on a research-peptide site looks a lot less like a shortcut and a lot more like a bet against yourself.
This guide is informational, not medical or legal advice. The compounded medications mentioned are not FDA-approved, and the approved options are prescription drugs requiring clinician screening. Anyone considering any of this should talk to a licensed clinician first.
Questions people are actually asking
Is it legal to buy weight-loss peptides online in 2026? It depends on which of the three lanes the product sits in. FDA-approved GLP-1 drugs like semaglutide and tirzepatide require a prescription through a licensed pharmacy. Compounded versions are legal through a licensed telehealth provider and a genuine prescription. “Research use only” peptides live in a gray area, and in 2026 the FDA made clear that the label doesn’t shield products that are obviously being marketed for people to take [2].
Could buying a “research use only” peptide and injecting it get someone in legal trouble? The bigger practical risk isn’t a knock on the door, it’s having no protections at all. The “research use only” label is the legal device that lets the product skip drug approval, so using it on yourself contradicts what the label says it’s for. There’s no clinician, no prescription, no licensed pharmacy standing behind the product, and no recall system if a batch turns out contaminated or mislabeled.
Why do legitimate sellers insist on a prescription before dispensing a GLP-1 product? Because that requirement carries the safety check built into the law. The approved semaglutide label includes a boxed warning for thyroid C-cell tumors and a contraindication for anyone with a personal or family history of medullary thyroid carcinoma or MEN 2 [4]. A clinician has to screen for exactly those risk factors before anything is dispensed. Skipping the prescription means skipping that screening, not saving anyone a step.
Is compounded semaglutide or tirzepatide the same thing as the brand-name drug? Not quite. The active peptide is the same, but the compounded product itself hasn’t been reviewed by the FDA for safety, effectiveness, or quality. It’s legal to obtain through the right channel, a licensed pharmacy and a real prescription, but it isn’t the FDA-approved drug. In 2026 the FDA warned 30 telehealth companies for marketing compounded GLP-1 products as though they were equivalent to the approved versions [3].
Are AOD-9604, 5-Amino-1MQ, MOTS-c, or tesofensine legal weight-loss treatments? None is FDA-approved for weight loss, so none is available as a legitimate prescription option. The only access point is the research-use-only channel, meaning every caution about that channel applies fully. Some also turn up alongside SARMs and are banned in tested sports, so being legal to possess and being allowed in competition are two different questions to clear.
What does the legitimate path to a weight-loss peptide actually look like? A licensed clinician, a genuine prescription, and a licensed pharmacy dispensing the product, whether brand-name or properly compounded. Most people get there through a telehealth provider, and how that provider describes compounding tells you a lot. Look for four things: a clinician consult first, a prescription requirement, a licensed pharmacy doing the dispensing, and honesty about what compounded medication is and isn’t.
What are peptides for weight loss, and how do they actually work?
They’re short chains of amino acids that mimic or stimulate hormones the body already makes, mainly GLP-1 and GIP, which govern hunger, blood sugar, and how fast the stomach empties. By binding to receptors in the gut and brain, they can reduce appetite and slow digestion. They aren’t stimulant-style fat burners. They work through hormones, which is a big part of why results vary so much depending on diet and lifestyle.
Is the safety risk around these peptides overblown?
Safety really comes down to which peptide, what dose, and where it was sourced. FDA-approved GLP-1 receptor agonists like semaglutide have years of clinical trial data, and the side-effect profile, mostly nausea and GI upset, is well documented. Research-chemical peptides bought online carry none of that: no purity guarantees, no dosing standards, no trial data. The danger often isn’t the molecule itself so much as the unregulated supply chain it came through.
What’s the best peptide for weight loss right now?
Based on current evidence, semaglutide and tirzepatide have the strongest human clinical data for meaningful, lasting weight loss, and both are FDA-approved under specific brand names for that purpose. Other peptides get plenty of enthusiastic attention online, but most lack placebo-controlled human trials at the doses actually being sold. Calling anything else “the best” right now would be getting ahead of the science, so sticking with what has cleared regulatory review is the safer bet.
Where can someone legally buy these peptides, and what makes a source legitimate?
Legally, the options are an FDA-approved prescription drug through a licensed pharmacy, or a compounded version prescribed by a physician and prepared by an accredited compounding pharmacy. A physician-supervised compounding setup, the kind FormBlends operates under, brings accountability, documented sourcing, and a licensed prescriber reviewing your health history. Sites selling peptides as research chemicals or supplements with no prescription required are operating in a legal gray area at best, and several have already faced FDA enforcement.
References
- Tirzepatide once weekly for the treatment of obesity (SURMOUNT-1): mean weight change −15.0% (5 mg), −19.5% (10 mg), −20.9% (15 mg) vs −3.1% placebo at 72 weeks. New England Journal of Medicine, 2022. https://pubmed.ncbi.nlm.nih.gov/35658024/
- FDA warning letter to Gram Peptides (MARCS-CMS 721806), dated March 31, 2026: retatrutide and tirzepatide offered as “research use only” are unapproved new drugs under section 505(a). https://www.fda.gov/inspections-compliance-enforcement-and-criminal-investigations/warning-letters/gram-peptides-721806-03312026
- FDA warns 30 telehealth companies against illegal marketing of compounded GLP-1 products. FDA press announcement, March 3, 2026.
- Semaglutide (Wegovy) prescribing information: boxed warning for thyroid C-cell tumors; contraindicated with personal or family history of medullary thyroid carcinoma or MEN 2. DailyMed.
- Retatrutide Phase 3 TRIUMPH-1: 12 mg dose −28.3% average body weight at 80 weeks vs −2.2% placebo. Eli Lilly, May 21, 2026.
Written by Priya Delgado, health explainer. Last reviewed January 2026.
This is background reading, not medical guidance. Your physician should make the final call.





